
SEPA Patient Focus – Upper Endoscopy
PATIENT’S GUIDE TO AN UPPER ENDOSCOPY
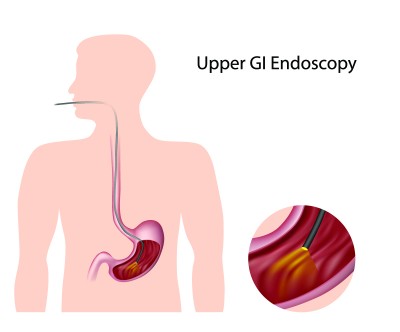
Your doctor has ordered an upper endoscopy. This procedure is performed by a gastroenterologist, surgeon or other trained professional. This test will examine the upper portion of your gastrointestinal track, which includes the esophagus, stomach and duodenum (first portion of the small intestine). Your doctor will use a thin, flexible tube called an endoscope, which has its own lens and light source, and will view the images on a video monitor. You might hear your doctor or other medical staff refer to upper endoscopy as upper GI endoscopy, esophagogastroduodenoscopy (EGD) or panendoscopy.
WHY IS AN UPPER ENDOSCOPY DONE?
Upper endoscopy helps your doctor evaluate symptoms of persistent upper abdominal pain, nausea, vomiting or difficulty swallowing. It is the best test for finding the cause of bleeding from the upper gastrointestinal track. It’s also more accurate than X-ray films for detecting inflammation, ulcers and tumors of the esophagus, stomach and duodenum.
Your doctor might use upper endoscopy to obtain a biopsy (small tissue samples). A biopsy helps your doctor distinguish between benign and malignant (cancerous) tissues. Remember, biopsies, are taken for many reasons, and your doctor might order one even if he or she does not suspect cancer. For example, your doctor might use a biopsy to test for Helicobacter pylori, the bacterium that causes ulcers.
Your doctor might also use upper endoscopy to perform a cytology test, where he or she will introduce a small brush to collect cells for analysis Upper endoscopy is also used to treat conditions of the upper gastrointestinal track. Your doctor can pass instruments through the endoscope to directly treat many abnormalities – this will cause you little or no discomfort. For example, your doctor might stretch (dilate) a narrow area, remove polyps (usually benign growths) or treat bleeding
HOW TO PREPARE FOR AN UPPER ENDOSCOPY The upper GI tract must be empty before upper GI endoscopy. Generally, no eating or drinking is allowed for 4 to 8 hours before the procedure. Smoking and chewing gum are also prohibited during this time. Patients should tell their doctor about all health conditions they have, especially heart and lung problems, diabetes, and allergies, and all medications they are taking. Patients may be asked to temporarily stop taking medications that affect blood clotting or interact with sedatives, which are often given during upper GI endoscopy. Medications and vitamins that may be restricted before and after upper GI endoscopy include:
- nonsteroidal anti-inflammatory drugs such as aspirin, ibuprofen (Advil), and naproxen (Aleve)
- blood thinners
- blood pressure medication
- diabetes medications
- antidepressants
- dietary supplements
Driving is not permitted for 12 to 24 hours after upper GI endoscopy to allow sedatives time to completely wear off. Before the appointment, patients should make plans for a ride home.
HOW IS UPPER ENDOSCOPY PERFORMED? Patients may receive a local, liquid anesthetic that is gargled or sprayed on the back of the throat. The anesthetic numbs the throat and calms the gag reflex. An intravenous (IV) needle is placed in a vein in the arm if a sedative will be given. Sedatives help patients stay relaxed and comfortable. While patients are sedated, the doctor and medical staff monitor vital signs. During the procedure, patients lie on their back or side on an examination table. An endoscope is carefully fed down the esophagus and into the stomach and duodenum. A small camera mounted on the endoscope transmits a video image to a video monitor, allowing close examination of the intestinal lining. Air is pumped through the endoscope to inflate the stomach and duodenum, making them easier to see. Special tools that slide through the endoscope allow the doctor to perform biopsies, stop bleeding, and remove abnormal growths. The doctor removes polyps and takes biopsy tissue using tiny tools passed through the scope. If bleeding occurs, the doctor can usually stop it with an electrical probe or special medications passed through the scope. Tissue removal and the treatments to stop bleeding are usually painless. The procedure usually takes between 15 and 60 minutes.
RECOVERY FROM UPPER ENDOSCOPY After upper GI endoscopy, patients are moved to a recovery room where they wait about an hour for the sedative to wear off. During this time, patients may feel bloated or nauseated. They may also have a sore throat, which can stay for a day or two. Patients will likely feel tired and should plan to rest for the remainder of the day. Unless otherwise directed, patients may immediately resume their normal diet and medications. Some results from upper GI endoscopy are available immediately after the procedure. The doctor will often share results with the patient after the sedative has worn off. Biopsy results are usually ready in a few days.
WHAT ARE THE RISKS OF UPPER ENDOSCOPY Risks associated with upper GI endoscopy include:
- abnormal reaction to sedatives
- bleeding from biopsy
- accidental puncture of the upper GI tract
Patients who experience any of the following rare symptoms after upper GI endoscopy should contact their doctor immediately:
- swallowing difficulties
- throat, chest, and abdominal pain that worsens
- vomiting
- bloody or very dark stool
- fever
AFTER UPPER ENDOSCOPY Most patients tolerate endoscopy very well and feel fine afterwards. Some fatigue is common after the examination, and you should plan to take it easy and relax the rest of the day. Your doctor can describe the result of the examination before you leave the endoscopy facility.
Click on image below to download your own printable copy of this handout
